HOW TO USE TIME IN RANGE (TIR) IN CLINICAL PRACTICE TO ASSESS GLYCEMIC CONTROL
TIR is metric that, together with Time Below Range (TBR) and Time Above Range (TAR), helps provide a more complete picture of a person’s glucose levels, enabling a more data-driven approach to glycemic control.1,2

Dr Alice Cheng, University of Toronto, discusses how TIR takes the guesswork away in diabetes management.
Healthcare professional has received a fee from Novo Nordisk Inc. for her participation.
Measured by continuous glucose monitoring (CGM), TIR can be used as a complement to hemoglobin A1c (HbA1c) in clinical practice.1,2 These 2 metrics may be used by healthcare professionals in combination to build personalized action plans to help improve daily glycemic control.1,2 This additional layer of insight offers the potential to drive meaningful conversations with people with diabetes around appropriate lifestyle adjustments, such as food choices and physical activity.1,2 The data may also help support healthcare professionals to make informed decisions on treatment choice, insulin dosage, and timing of doses.1,2
Clinical guidance and targets for TIR, a metric and complement to HbA1c in clinical practice.
TIR and HbA1c—working together to provide actionable insights
TIR and HbA1c provide actionable insights that can help empower people with diabetes and healthcare professionals to work together to improve glucose control and increase TIR.1,2 The table below is one representation of how TIR corresponds to HbA1c.2

The higher a person’s HbA1c, the higher their risk of developing diabetes-related complications.4-7 Increasing TIR corresponds to a decrease in HbA1c, with studies showing that for every absolute 10% change in TIR, there is an approximate 0.8% change in HbA1c.3
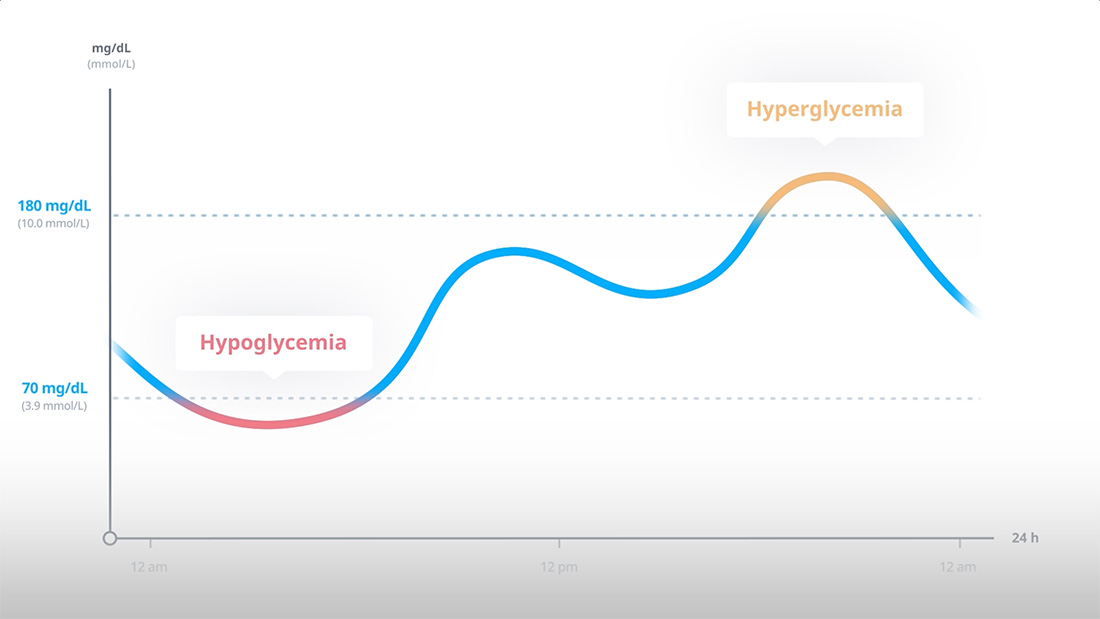
The International Consensus Report recommends that most people with diabetes should spend at least 70% of the day, or around 17 hours, in the target glycemic range of 70 to 180 mg/dL. This corresponds to the recommended HbA1c target of approximately 7%.1,2
TBR is the percentage of time spent below 70 mg/dL. Most people with diabetes should spend less than 4% of their day (1 hour) below range. TAR is the percentage of time spent above 180 mg/dL. Most people with diabetes should spend less than 25% of their day (6 hours) above range.1,2
- <1% of time (15 minutes) should be spent in the "very low" TBR of <54 mg/dL.1,2 This also applies to pregnant women with type 1 diabetes
- <5% of time (~1 hour, 12 minutes) should be spent in the "very high" TAR of >250 mg/dL1,2
- Battelino T, Danne T, Bergenstal RM, et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care. 2019;42(8):1593-1603.
- American Diabetes Association. Standards of Care in Diabetes—2023. Diabetes Care. 2023;46(suppl 1):S1-S291.
- Vigersky RA, McMahon C. The Relationship of Hemoglobin A1C to Time-in-Range in Patients with Diabetes. Diabetes Technol Ther. 2019;21(2):81-85.
- The relationship of glycemic exposure (HbA1c) to the risk of development and progression of retinopathy in the diabetes control and complications trial. Diabetes. 1995;44(8):968-83.
- Perkovic V, Heerspink HL, Chalmers J, et al. Intensive glucose control improves kidney outcomes in patients with type 2 diabetes. Kidney International. 2013;83;517–524.
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352: 837–53.
- The Action to Control Cardiovascular Risk in Diabetes Follow-On (ACCORDION) Eye Study Group and the Action to Control Cardiovascular Risk in Diabetes Follow-On (ACCORDION) Study Group. Persistent Effects of Intensive Glycemic Control on Retinopathy in Type 2 Diabetes in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) Follow-On Study. Diabetes Care. 2016;39:1089–1100.