
Victoza® is a once-daily GLP-1 RA therapy for patients with type 2 diabetes
Indicated as an adjunct to diet and exercise to improve glycemic control in adults and pediatric patients aged 10 years and older with type 2 diabetes and to reduce the risk of major adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke) in adults with type 2 diabetes and established cardiovascular disease.1
GLP-1 RA=glucagon-like peptide-1 receptor agonist
Victoza® efficacy and safety data for patients with type 2 diabetes
Interested in CV outcomes for patients also with established cardiovascular disease? Click here.
Adult study data
In a head-to-head study in adults with type 2 diabetes, Victoza® consistently outperformed Januvia®2
Primary endpoint: Mean change in A1C from baseline
After 26 weeks
Victoza® vs Januvia®
Pratley (1860)
Baseline A1C:
8.4% to 8.5%

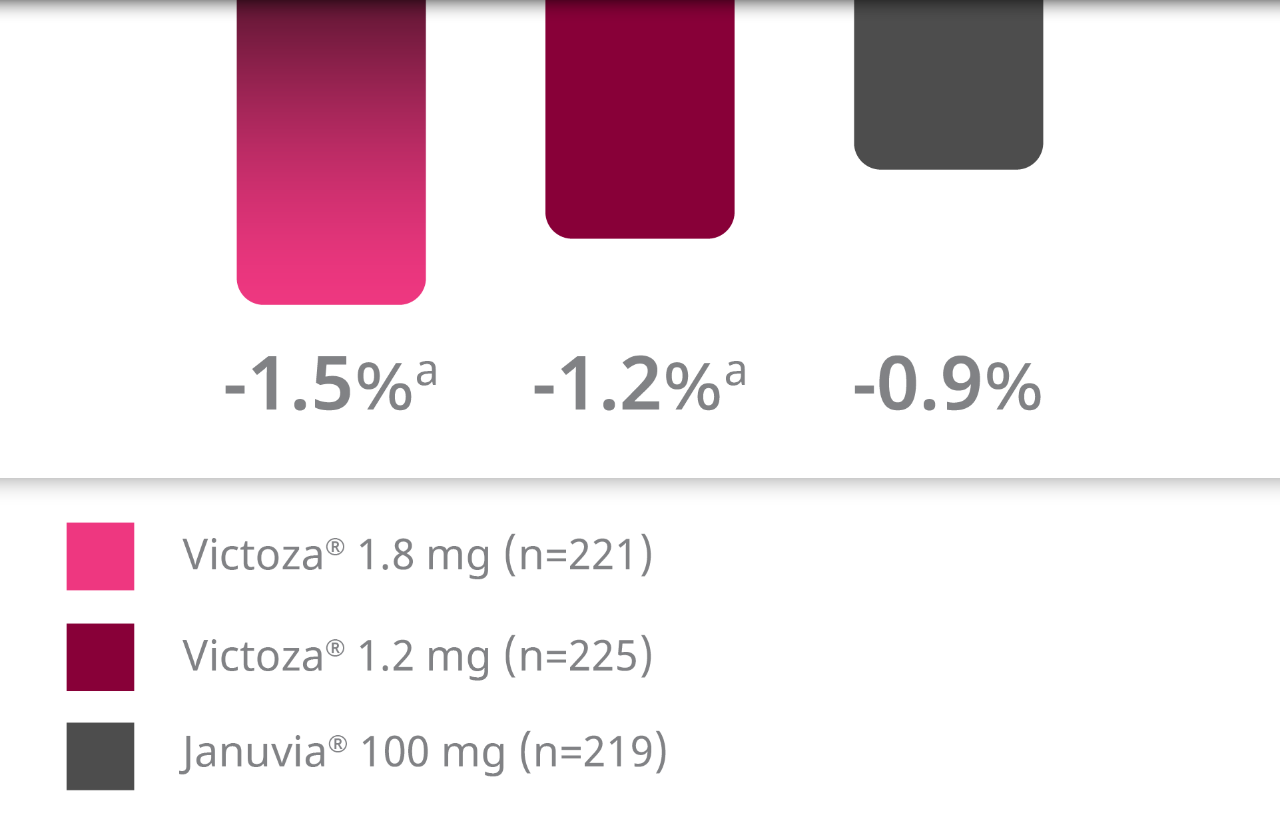
Studied in adults with type 2 diabetes taking metformin.
aP<0.0001 vs Januvia®.
In a head-to-head study in adults with type 2 diabetes, Victoza® was unsurpassed in A1C reduction vs Trulicity®3
Primary endpoint: Mean change in A1C from baseline
After 26 weeks
Victoza® vs Trulicity®b
AWARD-6
Baseline A1C:
8.1%


Studied in adults with type 2 diabetes taking OADs. Upper limit of the 95% CI (-0.19; 0.07) was less than prespecified noninferiority margin of 0.4%.
bStudy sponsored by Eli Lilly and Company.
In a head-to-head study in adults with type 2 diabetes, Victoza® demonstrated powerful A1C reductions after patients switched from Januvia®4
Primary endpoint: Mean change in A1C from baseline
After 26 weeks
Switch to Victoza® after Januvia®
Bailey (LIRA-SWITCH)
Baseline A1C:
8.2% to 8.3%


Studied in adults with type 2 diabetes taking metformin.
aP<0.0001 vs Januvia®.
Victoza® is not filtered by the kidneys5
In the LIRA-RENAL study, Victoza® showed no significant difference in renal function vs placebo as measured by eGFR, as a safety endpoint.6
Change from average baseline eGFR of 45 mL/min/1.73 m2:
-0.35 mL/min/1.73 m2
with Victoza® 1.8 mg (P=0.36)2
+0.37 mL/min/1.73 m2
with placebo2
No dosage adjustment recommended for patients with renal impairment1
There is limited experience with Victoza® in patients with end-stage renal disease.
Victoza® has not been found to be directly nephrotoxic in animal studies or clinical trials. There have been postmarketing reports of acute renal failure and worsening of chronic renal failure, which may sometimes require hemodialysis in Victoza®-treated patients. Some of these events were reported in patients without known underlying renal disease. A majority of the reported events occurred in patients who had experienced nausea, vomiting, diarrhea, or dehydration. Use caution when initiating or escalating doses of Victoza® in patients with renal impairment.
Victoza® provided significant A1C reductions over 26 weeks for adult patients with type 2 diabetes and moderate renal impairment6,c
Primary endpoint: Average A1C reductions
Baseline A1C
8.0% to 8.1%


cMild renal impairment=eGFR 60 to ≤89 mL/min/1.73 m2; moderate renal impairment=eGFR 30-59 mL/min/1.73 m2; severe renal impairment=eGFR <30 mL/min/1.73 m2.
dP<0.0001.
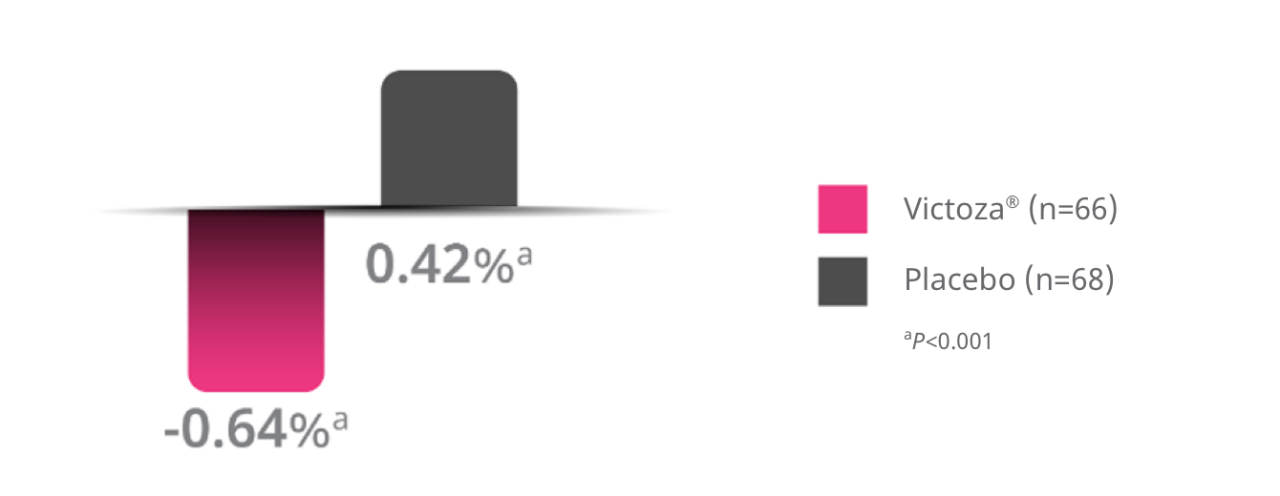
Victoza® was superior in reducing A1C from baseline versus placebo at 26 weeks1
Average adjusted A1C reductionsa
Victoza® + MET ± basal insulin
ELLIPSE
From mean baseline A1C:
7.7% to 7.9%
The change from baseline to end-of-treatment visit in A1C was analyzed using a pattern mixture model with multiple imputation. Missing observations (10.6% in Victoza®, 14.5% in placebo) were imputed from the placebo arm based on multiple (x10,000) imputations. The data for Week 26 were then analyzed with an ANCOVA model containing treatment, sex, and age group as fixed effects and baseline value as covariate.
Overall, the type and severity of adverse reactions in adolescents and children aged 10 years and above were comparable to those observed in the adult population.
In pediatric patients 10 years of age and older, the risk of hypoglycemia was higher with Victoza® regardless of insulin and/or metformin use.
A1C=glycated hemoglobin; CVD=cardiovascular disease; DPP-4=dipeptidyl peptidase-4; eGFR=estimated glomerular filtration rate; GLP-1 RA=glucagon-like peptide-1 receptor agonist; MET=metformin; OAD=oral antidiabetic drug; SU=sulfonylurea; T2D=type 2 diabetes.
CV outcomes for adult patients with type 2 diabetes and established cardiovascular disease
LEADER—a landmark CVOT for Victoza®1
9,340
patients
Key inclusion criteria:
T2D, A1C ≥7.0%
Age ≥50 years and established CVD
OR
Age ≥60 years and risk factors for CVD


Cardiovascular standards of care
(antihypertensives, lipid-lowering agents, and antiplatelet therapy)
Diabetes standards of care
(lifestyle modification, OADs, and insulin)
Duration 3.5-5 years
Time to first major adverse cardiovascular event (MACE) composed of:
Composite primary endpoint
CV death
Nonfatal MI
Nonfatal stroke

- Prospectively designed and powered to assess noninferiority and then superiority
- Patients were titrated to maximum tolerated dose of 0.6 mg to 1.8 mg
- Median daily dose of Victoza® was 1.78 mg
Victoza® significantly reduced MACE in adults with T2D and established CVD1

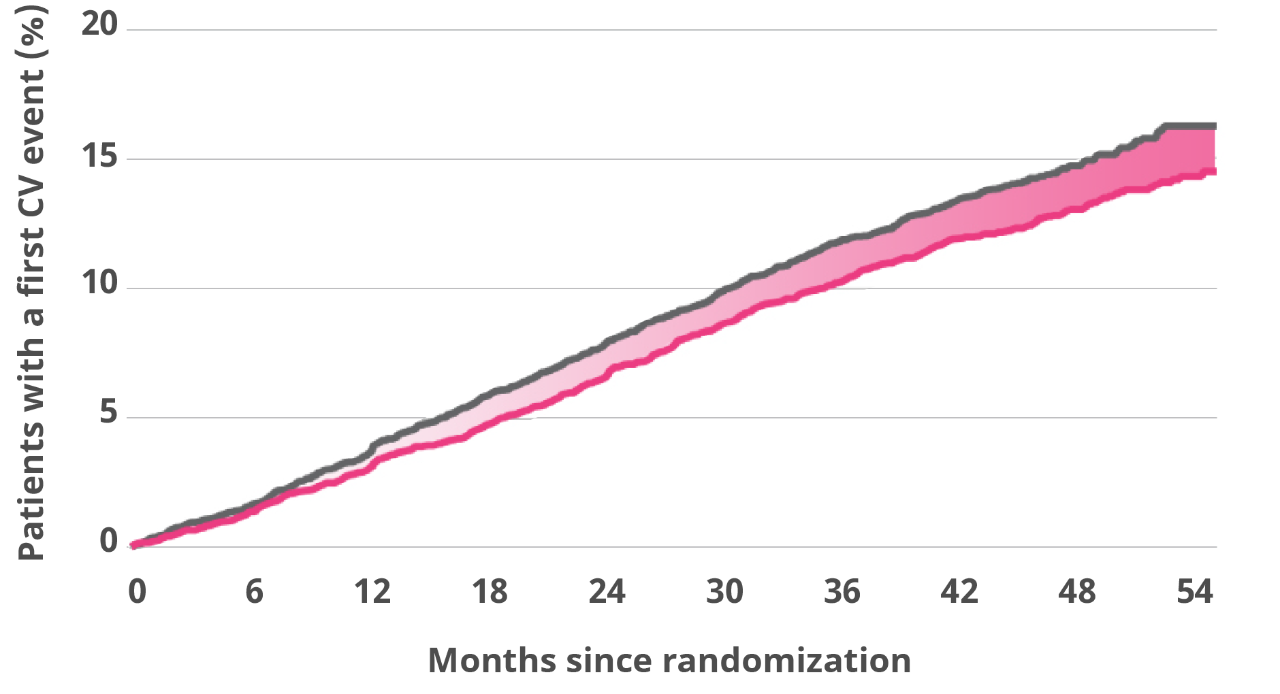
Absolute risk reduction:
1.9%
- Median time of exposure to treatment: 3.5 years.
- Median daily dose of Victoza®: 1.78 mg.
- The primary composite outcome occurred in fewer patients in the Victoza® group (608 of 4,668 patients [13.0%]) than in the SOC group (694 of 4,672 [14.9%]) (hazard ratio, 0.87; 95% confidence interval [CI], 0.78-0.97; P=0.01).
Victoza® provided a life-saving benefit1
Secondary endpoint: death from CV causes in adults with T2D as established CVD.


Death from CV causes was a prespecified secondary endpoint.
Hazard ratio, 0.78 (95% CI, 0.66-0.93).
Median time of exposure to treatment: 3.5 years.
Median daily dose of Victoza®: 1.78 mg.
Absolute risk reduction:
1.3%
Death from CV causes occurred in fewer patients in the Victoza® group (219 patients [4.7%]) than in the SOC group (278 [6.0%]) (hazard ratio, 0.78; 95% CI, 0.66-0.93).
Study designs
Pratley (1860)2
A 26-week, open-label, active-comparator, 3-armed, parallel-group trial to compare the efficacy and safety of Victoza® with sitagliptin for the treatment of type 2 diabetes in adults. Patients with type 2 diabetes inadequately controlled on metformin (N=665) were randomized to receive once-daily Victoza® 1.2 mg (n=225), Victoza® 1.8 mg (n=221), or sitagliptin 100 mg (n=219). The primary outcome was change in A1C.
Study-related adverse events
In a 26-week, open-label study in adult patients (N=665) comparing Victoza® 1.2 mg, Victoza® 1.8 mg, and sitagliptin 100 mg, all in combination with metformin, the adverse reactions reported in ≥5% of patients treated with Victoza® were nausea (23.9% vs 4.6%), headache (10.3% vs 10.0%), diarrhea (9.3% vs 4.6%), and vomiting (8.7% vs 4.1%).
(AWARD-6)3
A 26-week, randomized, open-label, parallel-group, multicenter (62 sites), multinational (9 countries), phase 3, noninferiority study. Patients were included based on the following criteria: adults with type 2 diabetes, treated with metformin, A1C of 7% to 10%, and a BMI of up to 45 kg/m2. Patients (N=599) were randomized to receive once-weekly Trulicity® 1.5 mg (n=299) or once-daily Victoza® 1.8 mg (n=300). The primary endpoint was change in A1C. Study sponsored by Eli Lilly and Company.
Study-related adverse events
The most common adverse events occurring in 5% or more of adult patients in the treatment groups combined (Victoza® 1.8 mg vs dulaglutide 1.5 mg): nausea (18% vs 20%); diarrhea (12% vs 12%); vomiting (8% vs 7%); dyspepsia (6% vs 8%); constipation (6% vs 4%); nasopharyngitis (7% vs 8%); headache (8% vs 7%); back pain (5% vs 4%); decreased appetite (7% vs 5%); and minor hypoglycemia (6% vs 9%). No major hypoglycemia occurred.
Bailey (LIRA-Switch)4
A 26-week, randomized, parallel-group, double-blind, double-dummy, active-controlled study to compare efficacy and safety in patients switching from Januvia® 100 mg to Victoza® 1.8 mg with patients who stayed on Januvia®. Adult patients with type 2 diabetes inadequately controlled on metformin (≥1500 mg/day) and Januvia® (100 mg/day) for at least 90 days prior to screening (N=407) were randomized 1:1 to switch to once-daily Victoza® 1.8 mg in addition to a Januvia® placebo or continued Januvia® 100 mg in addition to a Victoza® placebo, both in combination with metformin. The primary endpoint was a change in A1C.
Study-related adverse events
The adverse events most commonly reported in ≥5% of adult patients treated with Victoza® 1.8 mg vs Januvia® 100 mg, both in combination with metformin, were nausea (21.8% vs 7.8%), diarrhea (16.3% vs 9.3%), decreased appetite (8.9% vs 3.4%), vomiting (7.4% vs 4.9%), headache (6.4% vs 5.9%), nasopharyngitis (5.9% vs 3.4%), and increased lipase (5.5% vs 4.4%).
Davies (LIRA-RENAL)6
A 26-week, double-blind, placebo-controlled, parallel-group, randomized study in adult patients with type 2 diabetes and moderate renal impairment (eGFR 30-59 mL/min/1.73 m2). Patients were randomized to receive Victoza® 1.8 mg (n=140) or placebo (n=139) in addition to existing oral antidiabetics and/or insulin therapy. The primary endpoint was change in A1C. The insulin dose was reduced by 20% at randomization for patients with baseline A1C ≤8% and fixed until liraglutide dose escalation was complete. Dose reduction of insulin and SU was allowed in case of hypoglycemia; uptitration of insulin was allowed but not beyond the pretrial dose.
Study-related adverse events
Adverse reactions reported in ≥5% of patients and occurring more frequently with Victoza® compared with placebo included nausea (21.4% vs 4.4%), vomiting (12.1% vs 2.2%), diarrhea (7.1% vs 2.9%), constipation (5.7% vs 1.5%), increased lipase (15.0% vs 8.8%), GFR decreased (6.4% vs 5.1%), and headache (5.0% vs 2.9%).
ELLIPSE7
A 26-week, randomized, parallel-group, placebo-controlled trial with a 26-week double-blind period followed by a 26-week open-label extension. Eligible patients (N=135) between the ages of 10-17 years had A1C levels between 7%-11% if they were being treated with diet and exercise alone or between 6.5%-11% if they were being treated with metformin (with or without insulin) and had a body mass index (BMI) greater than the 85th percentile. Patients were randomized (1:1) to receive once-daily Victoza® (n=66) or placebo (n=68) for 26 weeks in combination with metformin with or without basal insulin on a background of diet and exercise regimen.
The treatment (Victoza® or placebo) was unblinded after the 26-week visit, and the trial was continued for an additional 26-week open-label extension. The basal insulin dose was decreased by 20% at randomization, and Victoza® was initiated at 0.6 mg/day and was titrated to 1.2 mg and 1.8 mg over the course of 2-3 weeks based on tolerability and an average fasting plasma glucose goal of ≤110 mg/dL. The primary endpoint was change in A1C from baseline at 26 weeks.
LEADER1
A phase 3b, multicenter, international, randomized, double-blind, placebo-controlled study to assess the cardiovascular safety of Victoza®. Adult patients with type 2 diabetes at high risk for cardiovascular events (N=9340) were randomized to receive once-daily Victoza® (0.6 mg-1.8 mg once daily with all patients being titrated to 1.8 mg once daily) or placebo. The primary endpoint was the time from randomization to a composite outcome consisting of the first occurrence of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke. The trial was prospectively designed and powered to assess whether Victoza® was noninferior or superior to placebo when measuring effect on CV events. Patients received trial products in addition to standard of care treatments such as oral antidiabetic treatments, insulin, and antihypertensive, antiplatelet, and lipid-lowering therapies.
Questions about dosing?
Learn more about prescribing Victoza®, and help your patients improve glycemic control.
Are you a pharmacist?
Looking for product information about Victoza®?
Important Safety Information for Victoza®
WARNING: RISK OF THYROID C-CELL TUMORS
- Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice. It is unknown whether Victoza® causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans, as the human relevance of liraglutide-induced rodent thyroid C-cell tumors has not been determined
- Victoza® is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC with the use of Victoza® and inform them of symptoms of thyroid tumors (eg, a mass in the neck, dysphagia, dyspnea, persistent hoarseness). Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with Victoza®
Indications and Limitations of Use
Victoza® (liraglutide) injection 1.2 mg or 1.8 mg is indicated as an adjunct to diet and exercise to improve glycemic control in adults and pediatric patients aged 10 years and older with type 2 diabetes and to reduce the risk of major adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke) in adults with type 2 diabetes and established cardiovascular disease.
- Victoza® should not be used in patients with type 1 diabetes
- Victoza® contains liraglutide and should not be coadministered with other liraglutide-containing products
Important Safety Information cont.
Contraindications
- Victoza® is contraindicated in patients with a personal or family history of MTC or in patients with MEN 2, and in patients with a serious hypersensitivity reaction to liraglutide or to any of the excipients in Victoza®. Serious hypersensitivity reactions including anaphylactic reactions and angioedema have been reported with Victoza®
Warnings and Precautions
- Risk of Thyroid C-cell Tumors: If serum calcitonin is measured and found to be elevated or thyroid nodules are noted on physical examination or neck imaging, the patient should be further evaluated
- Pancreatitis: Acute pancreatitis, including fatal and nonfatal hemorrhagic or necrotizing pancreatitis, has been observed in patients treated with Victoza® postmarketing. Observe patients carefully for signs and symptoms of pancreatitis (persistent severe abdominal pain, sometimes radiating to the back with or without vomiting). If pancreatitis is suspected, Victoza® should promptly be discontinued and appropriate management should be initiated. If pancreatitis is confirmed, Victoza® should not be restarted
- Never Share a Victoza® Pen Between Patients, even if the needle is changed. Pen-sharing poses a risk for transmission of blood-borne pathogens
- Hypoglycemia: Adult patients receiving Victoza® in combination with an insulin secretagogue (eg, sulfonylurea) or insulin may have an increased risk of hypoglycemia, including severe hypoglycemia. In pediatric patients 10 years of age and older, the risk of hypoglycemia was higher with Victoza® regardless of insulin and/or metformin use
- Acute Kidney Injury: Acute renal failure and worsening of chronic renal failure, which may sometimes require hemodialysis, have been reported postmarketing, usually in association with nausea, vomiting, diarrhea, or dehydration. Use caution when initiating or escalating doses of Victoza® in patients with renal impairment
- Hypersensitivity Reactions: There have been postmarketing reports of serious hypersensitivity reactions (e.g., anaphylactic reactions and angioedema) in patients treated with Victoza®. If a hypersensitivity reaction occurs, discontinue Victoza®; treat promptly per standard of care, and monitor until signs and symptoms resolve. Do not use in patients with a previous hypersensitivity reaction to Victoza®. Anaphylaxis and angioedema have been reported with other GLP-1 receptor agonists. Use caution in a patient with a history of anaphylaxis or angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be predisposed to these reactions with Victoza®
- Acute Gallbladder Disease: Acute events of gallbladder disease such as cholelithiasis or cholecystitis have been reported in GLP-1 receptor agonist trials and postmarketing. In the LEADER trial, 3.1% of Victoza®-treated patients versus 1.9% of placebo-treated patients reported an acute event of gallbladder disease, such as cholelithiasis or cholecystitis. If cholelithiasis is suspected, gallbladder studies and appropriate clinical follow-up are indicated
- Pulmonary Aspiration During General Anesthesia or Deep Sedation: Victoza® delays gastric emptying. There have been rare postmarketing reports of pulmonary aspiration in patients receiving GLP-1 receptor agonists undergoing elective surgeries or procedures requiring general anesthesia or deep sedation who had residual gastric contents despite reported adherence to preoperative fasting recommendations. Instruct patients to inform healthcare providers prior to any planned surgeries or procedures if they are taking Victoza®
Adverse Reactions
- The most common adverse reactions (incidence ≥5%) in clinical trials are nausea, diarrhea, vomiting, decreased appetite, dyspepsia, and constipation
- Immunogenicity-related events, including urticaria, were more common among Victoza®-treated patients (0.8%) than among comparator-treated patients (0.4%) in clinical trials
Drug Interactions
- Victoza® delays gastric emptying and may impact the absorption of concomitantly administered oral medications. Caution should be exercised when oral medications are concomitantly administered with Victoza®
- When initiating Victoza®, consider reducing the dose of concomitantly administered insulin secretagogues (such as sulfonylureas) or insulin to reduce the risk of hypoglycemia
Use in Specific Populations
- The safety and effectiveness of Victoza® have not been established in pediatric patients less than 10 years of age
- Victoza® slows gastric emptying. Victoza® has not been studied in patients with pre-existing gastroparesis
- Victoza® should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus
Please click here for Victoza® Prescribing Information, including Boxed Warning.
Reference:
- Victoza [package insert]. Plainsboro, NJ: Novo Nordisk Inc.
- Pratley RE, Nauck M, Bailey T, et al; for the 1860-LIRA-DPP-4 Study Group. Liraglutide versus sitagliptin for patients with type 2 diabetes who did not have adequate glycaemic control with metformin: a 26-week, randomised, parallel-group, open-label trial. Lancet. 2010;375(9724):1447-1456.
- Dungan KM, Povedano ST, Forst T, et al. Once-weekly dulaglutide versus once-daily liraglutide in metformin-treated patients with type 2 diabetes (AWARD-6): a randomised, open-label, phase 3, non-inferiority trial. Lancet. 2014;384(9951):1349-1357.
- Bailey TS, Takács R, Tinahones FJ, et al. Efficacy and safety of switching from sitagliptin to liraglutide in subjects with type 2 diabetes (LIRA-SWITCH™): a randomized, double-blind, double-dummy, active-controlled 26-week trial. Diabetes Obes Metab. 2016;18(12):1191-1198.
- Malm-Erjefält M, Bjørnsdottir I, Vanggaard J. Metabolism and excretion of the once-daily human glucagon-like peptide-1 analog liraglutide in healthy male subjects and its in vitro degradation by dipeptidyl peptidase IV and neutral endopeptidase. Drug Metab Dispos. 2010;38(11):1944-1953.
- Davies MJ, Bain SC, Atkin SL, et al. Efficacy and safety of liraglutide versus placebo as add-on to glucose-lowering therapy in patients with type 2 diabetes and moderate renal impairment (LIRA-RENAL): a randomized clinical trial. Diabetes Care. 2016;39(2):222-230.
- Tamborlane WV, Barrientos-Perez M, Fainberg U, et al. Liraglutide in children and adolescents with type 2 diabetes. N Engl J Med. 2019;381(7):637-646.